As the fall and back-to-school season progress, your child’s school-based speech therapy services are likely in full swing. At Speech Buddies, we believe parents should play an active and consistent role in their child’s therapy journey. Whether you’re new to therapy or have experience, this blog post offers a roadmap to help parents stay engaged, informed, and empowered throughout the process.
It All Starts with the Evaluation
For those new to therapy, the process starts with an evaluation to assess your child’s current skills and how they compare to age-matched peers. After receiving the evaluation report, schedule a call with the clinician to ensure you understand and agree with the findings. The report should provide a clear picture of your child’s strengths and areas for growth.
Ask the clinician to clarify the top priority goals and how they will be addressed, including whether they will focus on one or two goals at a time or multiple. Also, ask which goals are suitable for you to work on at home.
Materials!
Once your child’s therapy goals are clear and they’ve built a good relationship with their therapist, ask for simple, affordable materials to use at home, such as games, toys, or exercises. Choose fun items that make speech therapy enjoyable—these are likely the same activities their therapist uses to keep them engaged. Using familiar materials at home will help reinforce therapy goals. Let your child help pick the materials so they feel involved in the process. If cost is a concern, look into non-profits like Small Steps in Speech, which offer small grants to support therapy services or materials.
Progress Reports
School districts usually provide progress notes every six months or more often. Be sure to review these reports carefully, just like any other school report. If something doesn’t match what you’re seeing at home, or if you think there’s room for improvement, reach out to your child’s therapist and schedule a quick meeting. With over 20 years of experience, I can assure you that these conversations are important for your child’s progress and won’t be seen as overly demanding.
Achieving Goals and Sustaining Progress
Happily, your child will make significant progress and move on to more challenging and meaningful goals. As a parent or family member, you are a key player in solidifying those gains and making them habitual in your child’s speech and language. Think of your therapist as the leader, and you as the one who supports and strengthens the skills they have taught. While this is a vast topic covered in our Speech Buddies blog series, the underlying recommendation is to be consistent in follow-up exercises. Even a small daily commitment, like five minutes almost every day, can significantly help maintain the skills learned during therapy. Find a part of your family routine—like your commute, dinner time, or a homework reward—and designate it as your “speech practice time.” The key is to make it both convenient and consistent.
Congratulations on starting your child’s school-based speech therapy! These services are key to your child’s development and play an important role in their future. While the impact of therapy can vary, following the tips above will help you get the most out of it and have a positive effect on your child’s growth.
Gordy Rogers, M.S. CCC-SLP, & Speech Buddies Co-Founder
If a child shows concerning speech patterns, there is usually no clear cause. The vast majority of speech challenges related to development are what’s called idiopathic–they just happen. Sometimes, specific diagnoses can directly and casually affect speech challenges. Medical intervention can address these challenges, followed by intervention by a licensed speech-language pathologist.
Below, I summarize some of the most common issues related to otolaryngology (ear-nose-throat) that can present. Some may be present at birth and may be apparent or reveal themselves later in development; most issues appear in late toddlerhood or pre-school years. The goal of this post is to inform and empower parents and caregivers in a child’s development. However, it’s important to note that good care starts with qualified healthcare professionals.
Enlarged adenoids and tonsils
The adenoids, also known as pharyngeal tonsils, are bundles of lymphatic tissue that sit in the space between the oral and nasal cavities (the nasopharynx). When, after an infection like the common cold or an ear infection, the adenoids become inflamed (usually with pus–gross; I know), they can block proper nasal breathing. This issue can affect multiple vital systems in a developing child, but we’ll stick with speech here.
Often occurring in the later toddler years or during pre-school, enlarged adenoids can have varying effects on a child’s speech. Sometimes, there is no impact, while in others, it can be profound and require immediate attention. Speech affects include hyponasal speech, where children sound stuffed up. This can lead to a habitual open-mouth breathing posture, which can lead to changes in how a child articulates speech sounds.
The adenoids are the most likely to affect a child’s speech development when inflamed, but the palatine and lingual tonsils are also important to consider. When you open your mouth wide, you can see the palatine tonsils on the back sides. The lingual tonsils, not visible, are at the base of your tongue (see picture). These two tonsils affect speech production only when inflamed.
Should you suspect that your child’s adenoids and/or tonsils are affecting speech development, the first course of action would be to consult with your pediatrician or pediatrician otolaryngologist. A course of antibiotics and/or oral steroids can solve the problem. In rarer cases, surgery is required. Urgency is crucial, as delays can worsen speech problems. Please also see a previous blog post on this subject. (Tonsils & Adenoids)
I’ll be brief and direct you to this blog post (Is My Child Tongue-Tied?) as this subject is important and a current topic of discussion. There has been an uptick in the number of tongue tie surgeries being performed. The procedure is often quick, straightforward and painless when performed by a qualified provider such as an otolaryngologist or specialized pediatric dentist.
Parents should understand that the severity of tongue tie can affect speech and other oral behaviors like feeding and swallowing. I have seen unsubstantiated (and wild) claims from certain providers stating that tongue tie surgery can improve symptoms of autism and stuttering. Healthcare consumers must tread cautiously and remain vigilant against such claims, ensuring they comprehend the motives of those advocating for this procedure. Throughout my nearly twenty-year clinical practice, I have observed the changing opinions of clipping the lingual frenulum, with periods of powerful encouragement followed by periods of strong discouragement. Having a perspective that attitudes can swing based on recent evidence is crucial.
That said, tongue tie can have a negative impact on a range of critical behaviors, like suckling/breastfeeding, oral feeding, swallowing and speech. Any situation that limits a child’s tongue range of motion can affect functioning. As with adenoids and tonsils issues, the first line of defense, so to speak, is to consult with your pediatrician and ask him/her for a specialist referral.
Lip tie (sometimes referred to as bugloss)
As the name implies, lip tie occurs when the labial frenulum limits the range of motion of the lips. This condition less commonly affects speech development and production. When it does, the lip tie is usually quite severe. However, certain speech sounds require precise lip movements and lip tie. Again, as with tongue tie, should you suspect this is occurring in your child, your first course of action would be to contact your pediatrician.
Velopharyngeal insufficiency
Separating the mouth and nose is necessary for numerous reasons, too many to detail here. Compromising this separation can affect speech (and other functions). The hard palate, a piece of the maxilla (upper jaw) bone that fuses while a child is in utero, separates the mouth (oral cavity) and nose (nasal cavity). Sometimes, the incomplete fusion results in a cleft palate. Pediatricians almost always diagnose this condition at birth. They have a comprehensive, stepwise plan to treat and facilitate your child’s proper development of structures and functions.
Sometimes, however, an anatomical issue may be less apparent (i.e., a submucosal cleft). In these cases, a child’s voice might sound unusual, often hypernasal where air is escaping out of the nose when it shouldn’t. This issue requires a full clinical workup and diagnosis from a specialized physician. The course of treatment and speech therapy may vary for a congenital palate issue.
Finally, a situation can arise where velopharyngeal insufficiency occurs because the soft palate cannot function or may have malformations or injuries. The soft palate is a flap of muscle tissue between the nasal and oral cavities that raises and lowers to open or close off the nasal cavity. Just as with hard palate issues, soft palate challenges can make a child’s speech hyponasal. If the challenge is anatomical, the pediatric otolaryngologist will again possess the best resources to chart a course of treatment.
With these conditions, time is of the essence! Children have what we call critical periods for specific skills, like speech. Their brains are most receptive to learning these skills during specific age ranges. For speech, this occurs from birth to around 8-9 years old. Although it’s possible for a child to develop crucial speech skills after age 8-9, progress might be slower and therapy programs more complex and challenging. No matter your concern, the first step is to get information from a local licensed medical or speech and language professional. At Speech Buddies, we would be honored to assist you!
Gordy Rogers, M.S. CCC-SLP, & Speech Buddies Co-Founder
When the American Medical Association Speaks, We Listen
I’ve been quite affected by a recent research study published in the Journal of the American Medical Association (JAMA). The research aimed at answering this question: did the Covid-19 pandemic affect the rate of diagnosis of speech delay in children up to the age of five?
The answer was a clear yes. The pandemic did see a great frequency of diagnosis of speech delay in children.
This post is dedicated to acknowledging this reality and proposing solutions to the collateral effect of the pandemic.
Study Key Points:
First, the study was huge. The authors’ analysis covered almost 2.5 million children. They were broken into four groups, one year-olds, two year-olds, three year-olds and four year-olds.
Second, the results were statistically significant. The researchers can be very confident that their findings are not due to chance and are in fact a representation of reality.
Third, they found increased diagnosis across all four age groups analyzed.
Solutions:
Now that we understand this situation is real and the pandemic is the likely cause of a greater prevalence of speech delay, let’s talk about what we can do to address it.
When a parent, teacher or pediatrician first raises a concern about a child’s speech development, the first step is always an evaluation with a licensed speech-language pathologist. Should the evaluation yield a diagnosis of speech delay, the next urgent step is to begin a course of therapy.
For decades, we’ve known of the existence of critical periods of speech development. The periods that children are expected to acquire given skills by a certain age. If a child misses these critical windows of development, rest assured speech therapy has been proven to catch children up. However, the sooner a child can be seen, the better the child’s prognosis.
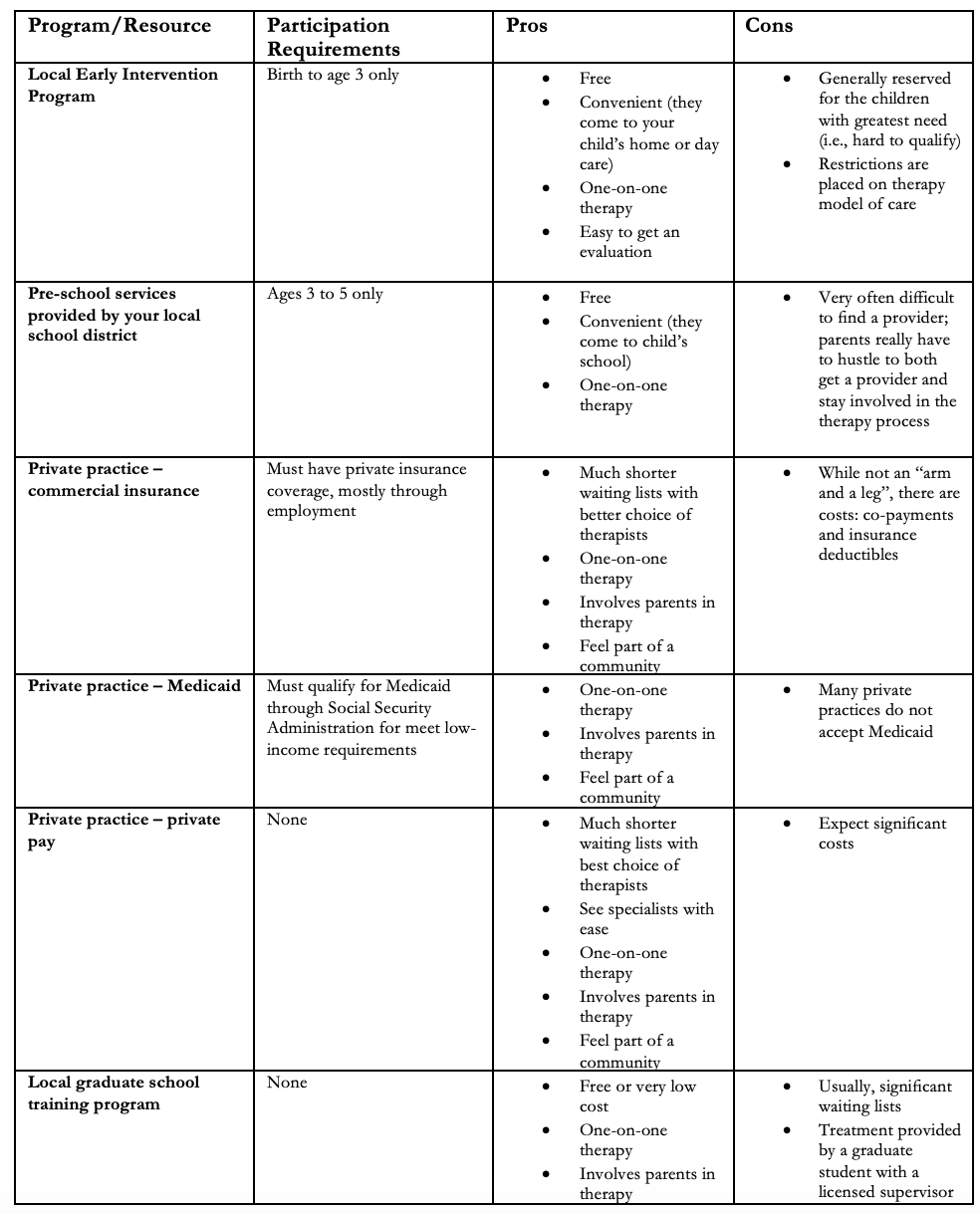
Once a decision is made to get an evaluation, the next question to answer is where will we get these services? Luckily, there are many ways to do this but they all require a different procedure and have their strengths and drawbacks.
Options to explore:
See below for a list of these options which may be dependent on age, income or employment requirements:
This list is not absolutely exhaustive and other options that may be available to you. Here are a few examples:
Grant funding TriCare (military insurance) Therapeutic day schools – more significant developmental or medical needs
Connect:
At Speech Buddies we are committed to providing superior speech therapy solutions for all involved in the process (children, parents, caregivers, educators and fellow therapists).
Our Speech Buddies Tools have strong data to support their use with a wide range of speech delays. We also offer a free online directory for speech therapists nationwide on Speech Buddies Connect.
Lastly, we know the importance of setting up speech therapy promptly following a speech delay diagnosis. Please feel free to email us at info@speechbuddies.com for guidance on how to get started. We’d welcome the opportunity to point you in the right direction of either local, regional or national resources that you’d have available to you.
December 4, 2023 Brianna M. Goodwin Cartwright, MS1; Peter D. Smits, PhD1; Sarah Stewart, MD1; et al Patricia J. Rodriguez, PhD, MPH1; Samuel Gratzl, PhD1; Charlotte Baker, DrPH, MPH, CPH1; Nicholas Stucky, MD, PhD1 JAMA Pediatr. 2024;178(2):193-195. doi:10.1001/jamapediatrics.2023.5226
In my clinical career, I have direct comparisons of parents who were deeply involved in their children’s therapy regimen and those who were not. In almost every case, the parents who were more involved in their child’s speech regimen had the most success.
Here are several tips for how you can be the ideal partner in your child’s therapy process.
Ask Questions – Starting from your child’s initial evaluation through every stage of therapy, don’t be afraid to ask your speech therapist questions. Make sure you understand the recommendations given in your child’s evaluation report. Whenever therapy goals are listed, ask about the rationale behind each goal and the sequence of those goals. Will they target goals individually or several at once? Inquire about your child’s progress after a few weeks of therapy. What goals is your child most naturally making progress with? What activities are your child most motivated by? And what the discharge plan is. Your therapist will appreciate your active involvement in the therapy process, even if it seems like micro-managing.
Offer Suggestions – Don’t be afraid to offer suggestions to your therapist. You will defer to your experienced, licensed professional regarding therapy techniques, goal selection, and the key clinical considerations. However, it is essential that your therapist know what brings your child joy. This can include games or activities that motivate your child, their preferred feedback or reinforcement (i.e. after each correct answer or at the end of a block of items), and potential prizes. Therapy should always be fun and focus on connecting with your child and their interests. Most therapists are well-stocked with games and other reinforcement tokens but, imparting your knowledge of what makes your child tick will pay enormous dividends for their growth.
Practice Makes Perfect – This adage applies in almost every area of speech and language therapy. There’s no need to do more than your family can reasonably take on. However, research strongly suggests that frequent short home-based “sessions” are the ideal way to pursue follow-up exercises. For example, three to four times per week for ten to fifteen minutes per session. Definitely take your therapist’s lead and refrain from doing activities or exercises that aren’t “assigned” by your therapist. When in doubt, ask for direction or clarification from your therapist.
It’s a Process – Speech and language therapy isn’t a linear process. I’ve seen early strong progress turn to mid-therapy frustration and vice versa. I’ve seen minimal early progress give way to rapid change just as everyone was throwing their hands up in frustration. The lesson here is it’s probably prudent to expect at least several months of visits, depending on the nature and number of goals on your child’s therapy plan.
Speech and language are complex behaviors that can require time, persistence, and thoughtful intervention to change. In many cases, there’s simply no way around this. By following the guidelines I’ve provided, you can make therapy more efficient and ensure a positive experience for your family.
As parents, my wife and I always try to perform cost-benefit analysis when our kids need professional or healthcare services. We all want the best for our children, but is that service worth the cost? This question often boils down to determining if it’s the right time for these services.
I’ll provide clarity on this important decision using an impactful research study. My goal is to help you better perform your own cost-benefit analysis when you feel your child may need a speech evaluation.
It’s important to understand that this article is devoted to speech clarity errors rather than language or cognitive development. I’m not addressing speech fluency here; one of the most common disorders being stuttering.
In 2018, two prominent Australian researchers and speech-language pathologists, Sharynne McLeod and Kathryn Crowe, published a highly influential study which looked into 27 major languages, on the ages that children are expected to acquire the speech sounds of their language.
Before this study was published, most speech pathologists relied on now fifty-year-old data to help determine whether the speech errors a child was making were age-appropriate (i.e. “normal” for that age group) or suggestive of a speech disorder. McLeod and Crowe’s data sent shockwaves through the world of speech pathology.
Speech pathologists thought that some of the trickiest-to-learn speech sounds can be misarticulated up to age 7, or even 8, without triggering a concern. The old data suggested therapists should recommend a “wait and watch” approach for a child who couldn’t pronounce [r] or [th] sounds at age 7.
One common issue is [th] and [r] are produced incorrectly in a 7-year-old that a good percentage of these children would spontaneously correct these speech errors without therapy.
McLeod and Crowe’s study examined many previous studies (termed a meta-analysis) and changed this thinking. They found that 90% of the speech sounds in a language should be acquired (i.e. correctly produced) by age 5! So whereas in years past, a 5 and a half-year old presenting with a challenge in saying his/her [s] and [sh] sounds might be told to wait a year before going to therapy, this new guidance would more strongly support intervening right away.
Each case is unique and is best informed by a comprehensive speech evaluation by a trained Pathologist. However, McLeod and Crowe’s work suggests a more proactive approach earlier in a child’s development. This applies broadly to children’s speech development as well.
Knowing language history, bilingualism, and family speech disorders is critical for clinical decision making. This boils down to a maxim: when in doubt, evaluate!
This study further underscores the potential urgency of the situation. The watchful waiting approach may actually be the best one, but you won’t know that without getting all the facts.
Best of luck in your family’s speech journey. Please share this article with someone who needs help with determining when the time is right for a professional speech evaluation.
By Gordy Rogers, M.S. CCC-SLP
**References “Children’s Consonant Acquisition in 27 Languages: A Cross-Linguistic Review” by Sharynne McLeod and Kathryn Crowe
Ahhh summer. The time of year when your child’s speech plan is interrupted because of camp and family vacations. As much as our kids deserve a break from their academic routine, pausing can affect your child’s momentum toward his/her speech goals.
Speech Buddies® can maintain and progress speech skills over the summer, regardless of the learning phase or service provider.
Phases of speech development:
1. The Establishment Phase – With the help of his/her therapist the child is learning to unlearn previous patterns of speech production. If your child is in this phase, it’s crucial to include frequent practice sessions with the Speech Buddies tools. By feeling the correct placement of the tongue in a variety of speech contexts, summer practice with Speech Buddies can be directed, effective and very efficient. Just five to ten minutes per day is beneficial.
2. The Generalization Phase – In this phase, the sound has already been established, but your child still requires these new speech skills to become a habit in everyday speech.
Our tools help orient your child’s entire sound system to the proper placement and movement of the challenge sound (s). We offer carefully developed supplementary materials to support your home-based programming. Find our free lesson plans here.
Applying a framework like Speech Buddies can provide structure and direction to your home-based work with your child; just getting going and sticking with a program is half the battle.
Kids deserve their summers to explore, to experiment, and unwind. Yet, with Speech Buddies, summers can also be a time of growth through practice without it feeling like work.
Visit our website or contact us to help with your family’s summer speech program!
The Covid pandemic brought an unprecedented staffing challenge across the entire American healthcare system. From hospitals, to outpatient private practices to schools, there aren’t enough speech pathologists to serve the demand for services that further exploded because of lockdowns.
We are seeing research studies come out now that confirm how lockdowns and remote learning set children back in their speech development.
While this might explain why your child hasn’t been receiving the school-based or clinic-based services, it does nothing to allay your concerns as a parent.
But with the help of Speech Buddies®, you can take your child’s speech development into your own hands.
Let me explain.
Speech Buddies are a set of patented, clinically proven hand-held devices that help a child feel correct tongue placement for those most difficult speech sounds that typically develop in late pre-school and early school years.
Since 2007? thousands of speech pathologists and tens of thousands of parents and children have successfully used them. See our testimonials here. Speech Buddies takes the guesswork out of eliciting speech sounds and speed up a child’s acquisitions of these often difficult-to-learn speech sounds.
The elegance of Speech Buddies as a speech therapy solution lies both in its efficacy and flexibility.
We always recommend having your child evaluated and treated by a licensed speech pathologist for a diagnosed speech challenge, especially if you believe your child’s speech challenge may be more than just of mild severity.
But, Speech Buddies may provide a critical bridge to expedited care amid this staffing situation. You may have an “ah ha moment” within the first few minutes of using the device and our extensive library of training videos and lesson plans will give you a head start on your child’s treatment regimen.
Because we specifically designed Speech Buddies tools for each speech sound (please see descriptions of each device: R, S, SH, L, CH), you only need to purchase the device(s) that apply to your child’s situation. So, when you’re finally moved off the waiting list for services, you could be farther along in the therapy process.
Depending on the speech therapy staffing predicament in your local area, Speech Buddies may also offer a fantastic option for those who would opt for out-of-network services, resources permitting, while potentially reducing the overall cost of those services.
Out-of-network providers almost never have extensive waiting lists given very limited or unavailable funding coverage.
You should be able to get in for an evaluation and services without being placed on a waiting list. If Speech Buddies work for your child’s speech treatment regimen, our tools are proven to reduce the time in therapy for certain speech sound disorders. By accessing a key sensory modality in learning, the sense of touch, Speech Buddies can help achieve a quicker learning breakthrough.
Speech Buddies hand-held tool empowers both the parent and child to recreate the speech therapy session in your own home while building confidence and enabling critical parent involvement in therapy. We also offer a free directory, Speech Buddies Connect, of SLP’s on our website.
Parents are powerless over staffing challenges across healthcare services but, you have access the clinically proven options.
Your child’s speech development is important and can be complex. If you ever have questions about Speech Buddies as a specific solution for your child’s situation, please contact us today!
We’re happy to hear your child’s situation and point you toward actionable solutions.
1. What inspired you to become a speech therapist? My grandmother was the matriarch of the family. In 1991 she fell ill due to a stroke and I saw how therapists, especially a speech language pathologist, came to improve her quality of life.
2. What do you love about being an SLP? I love helping children find their voices.
3. What is your SLP superpower? Patience. Not all clients I work with are happy to see me. I have found that when you take the time to find out what your client likes it makes a difference in the service provided.
4. Who do you find the most rewarding to work with? The majority of my most rewarding clients to work with are under the age of 10. They usually make the most improvement in shorter periods of time. Though parents might be excited to her their child speak for the first time, I find it to be a honor to hear a child who was completely nonverbal, now talk: all from a strategy I used.
5. What would you say to parents who have a child with a speech challenge? Offering developmental norms helps tremendously. It helps the parent understand what should be addressed as well as why. The idea for me is to keep your child within the expected milestones for communication skills.
6. What is the most challenging thing about being a kid with a speech challenge? I think children become frustrated when they do not make progress. This can be especially hard as they mature.
7. What is one question you get most often from clients and parents? Most parents ask, in various ways, “How old are you?”, since I look much younger than I am. My work experience as a Speech Language Pathologist began in 2010.
8.What advice would you like to give to families considering seeking speech services? My best advice is seek evidence based information about your child’s needs before you reach out to any service provider. The best resource for a parent seeking a Speech Language Pathologist is the American Speech-Language & Hearing Association, ASHA. There are many sources that give information that is false or not proven. It can make it hard to work with your therapist (of any training) if you come in expecting one thing and what is realistic is what your therapist is offering you.
9. I’m sure you’ve had many, but what is one of your most memorable or rewarding cases and why? My most memorable case was one where the client was completely noncompliant during an evaluation. The client I am referring to stood up on the table at home and would not allow me to complete the assessment I attempted to administer. This client’s parent was determined to have the evaluation complete and I did my very best. This client is almost a completely different child now. The client is able to combine words, sits to attends tasks, and is making good progress towards mastering speech goals.
10. What can clients expect from virtual therapy? What is different or beneficial about virtual therapy? Virtual therapy is an option for patients in areas where a Speech Language Pathologist might not be accessible. It is an ASHA approved way to provide services. The expectation should be the same as face to face speech therapy. Some considerations for virtual speech therapy are that your internet connection should be supplemented with a USB cable. It is difficult, but not extremely impossible to offer PROMPT over virtual speech therapy: some patients pick up visual cues well. An e-helper is often needed for younger patients to receive the service.
11. What is your favorite part of being a Speech Buddies Connect therapist? My favorite part of working with Speech Buddies Connect is that I am not paperwork driven. There is time that I am able to sit with parents to go over progress then offer carryover.
Calling all Speech Buddies readers! We want to hear from you. What Mommy blogs do you read? What blogs are your favorite? Let us know for your chance to win a free set of Speech Buddies flashcards.
As children grow and their language develops, they learn more than just words. They learn about the world around them and how to socialize with different people in different contexts. They learn how to adapt their behavior depending on their conversation and social environment. These rules of communication are called pragmatics, and will vary depending on the development and culture of the child. Kindergartners will behave very differently on the playground than in the classroom. Likewise, preschoolers in Japan and France may have different social communication expectations placed on them. While the United States remains a melting pot of many different cultures, research shows some common benchmarks in the development of social communication. And while it’s important to remember that all children may develop at their own pace, growth of these social skills is important for both social and academic success.
Our eyes can reveal a lot about us and our social use of eye contact is a vital act of communication. They can reveal whether we are interested or distracted, whether we are telling the truth or a lie and suggest how confidence we feel. This is why it is important for children to develop a communicative competence through appropriate eye contact in order to become better engaged with others. Children begin learning pragmatics at birth and continue to develop these skills throughout life. Within the first year, typically developing children will show social communication with eye contact, vocal turn taking, and facial expression and recognition. As they develop, children will continue to learn from their environment, and begin to understand pragmatic rules and social clues. Children with disorders like autism tend to have significantly reduced eye contact than is considered socially accepted. This may lead communication partners to misinterpret their reduced eye contact as a lack of interest; often, the “rules” of eye contact in a social context are difficult to master for this population. Understanding social thinking, as well as the inherent challenges certain children may face here, can help build meaningful relationships.
Pragmatics and Neurodevelopmental Disorders
It is important to remember that children with neurodevelopmental disorders will display a number of developmental “red flags”, and not every child will have the same presentation. If you are concerned that your child is not meeting these milestones, you may want to consult with your pediatrician. If your child is then diagnosed with a social communication deficit, speech therapy can be an important piece of their intervention plan. Speech-language pathologists (SLPs) are not only experts on speech and language development, but also nurture the social and emotional growth of their clients. Children who struggle to make eye contact and other social communication challenges often benefit from group therapy, where they can interact with like peers who are working on the same or similar goals in a format moderated by the SLP. SLPs may also use cognitive behavioral therapy to help reduce anxiety and negative thoughts associated with social communication in order to help clients self regulate and process emotions. Additionally, SLPs work collaboratively with other specialists such as occupational therapists and therapists trained in Applied Behavior Analysis (ABA). There are many different approaches to therapy and it may take time to determine which approach, or combination of approaches, is right for your child. So continuing to educate yourself as a parent will help you make the both informed clinical decisions as well as maximize your effectiveness as a home-based partner in your child’s total therapy program.












 1. What inspired you to become a speech therapist? My grandmother was the matriarch of the family. In 1991 she fell ill due to a stroke and I saw how therapists, especially a speech language pathologist, came to improve her quality of life.
1. What inspired you to become a speech therapist? My grandmother was the matriarch of the family. In 1991 she fell ill due to a stroke and I saw how therapists, especially a speech language pathologist, came to improve her quality of life.